


Patient care can become complex. Multiple chefs in the kitchen, so to speak. Sparse medication reconciliation. Going from patient to patient. Top it off with a variety of medications on board.
A patient visits reporting swelling in their legs. Patients are unofficially trained to expect a prescription for each concern or at each appointment. They request something to help with the swelling. There’s an easy fix to this – furosemide to the rescue. The swelling subsides, the patient is satisfied.
Eventually the patient returns, this time complaining of frequent urination. They request a prescription to help. Easy enough – one is written for their overactive bladder, Oxybutynin. The patient is satisfied. The provider did their job and fixed the problem.
While this scenario is highly simplified, the prescribing cascade continues to expand. Interesting enough, the originating culprit remains in place – the patients current prescription for amlodipine. The swelling was in result to the calcium-channel blocker. The added solution, furosemide, became a culprit as well – frequent urination. The cascade could continue on, unfortunately as urinary incontinence medications have a whirl-wind of possible adverse drug reactions as well.
Pharmacists are trained to watch for this type of scenario. A adequate and fully assessed medication reconciliation can proactively reduce these cascades. Integrating a pharmacist into the patient-care model can also retroactively assess for appropriateness of therapy of each medication. There continues to be ample opportunity to de-escalate patients medication regimens with assistance from a pharmacist.
Prescribing cascades
Patient care can become complex. Multiple chefs in the kitchen, so to speak. Sparse medication reconcilliation. Going from patient to patient. Top it off with a variety of medications on board.
A patient visits reporting swelling in their legs. Patients are unofficially trained to expect a prescription for each concern or at each appointment. They request something to help with the swelling. There’s an easy fix to this – furosemide to the rescue. The swelling subsides, the patient is satisfied.
Eventually the patient returns, this time complaining of frequent urination. They request a prescription to help. Easy enough – one is written for their overactive bladder, oxybutnin. The patient is satisfied. The provider did their job and fixed the problem.
While this scenario is highly simplified, the prescribing cascade continues to expand. Interesting enough, the originating culprit remains in place – the patients current prescription for amlodipine. The swelling was in result to the caclium-channel blocker. The added solution, furosemide, became a culprit as well – frequent urination. The cascade could continue on, unfortunately as urinary incotinence medications have a whirl-wind of possible adverse drug reactions as well.
Pharmacists are trained to watch for this type of scenario. A adequate and fully assessed medication reconcilliation can proactively reduce these cascades. Integrating a pharmacist into the patient-care model can also retroactively assess for appropriateness of therapy of each medication. There continues to be ample opportunity to de-escalate patients medication regimens with assistance from a pharmacist.
Can we put a image with arrows? ????
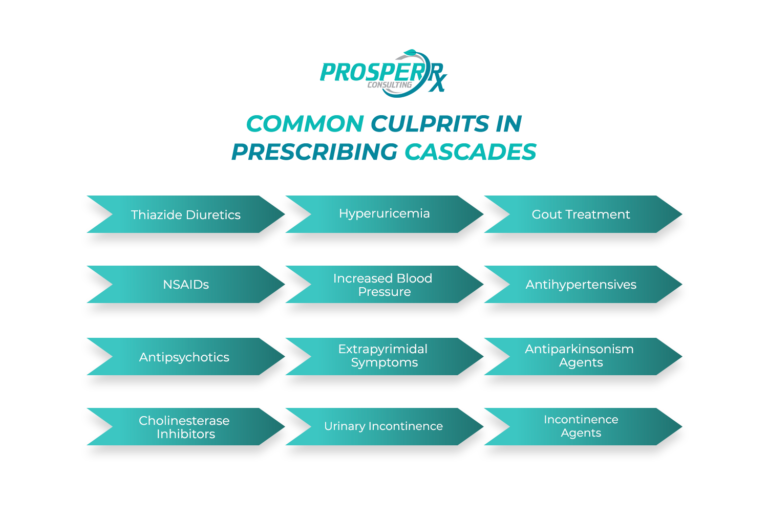
Common culprits in prescribing cascades
Thiazide diuretics –> Hyperuricemia –> Gout treatment
NSAIDs –> Increased blood pressure –> Antihypertensives
Antipsychotics –> Extrapyrimidal Symptoms –> Antiparkinsonism agents
Cholinesterase inhibitors –> Urinary Incontinence –> Incontinence agents
Prescribing cascades
Patient care can become complex. Multiple chefs in the kitchen, so to speak. Sparse medication reconcilliation. Going from patient to patient. Top it off with a variety of medications on board.
A patient visits reporting swelling in their legs. Patients are unofficially trained to expect a prescription for each concern or at each appointment. They request something to help with the swelling. There’s an easy fix to this – furosemide to the rescue. The swelling subsides, the patient is satisfied.
Eventually the patient returns, this time complaining of frequent urination. They request a prescription to help. Easy enough – one is written for their overactive bladder, oxybutnin. The patient is satisfied. The provider did their job and fixed the problem.
While this scenario is highly simplified, the prescribing cascade continues to expand. Interesting enough, the originating culprit remains in place – the patients current prescription for amlodipine. The swelling was in result to the caclium-channel blocker. The added solution, furosemide, became a culprit as well – frequent urination. The cascade could continue on, unfortunately as urinary incotinence medications have a whirl-wind of possible adverse drug reactions as well.
Pharmacists are trained to watch for this type of scenario. A adequate and fully assessed medication reconcilliation can proactively reduce these cascades. Integrating a pharmacist into the patient-care model can also retroactively assess for appropriateness of therapy of each medication. There continues to be ample opportunity to de-escalate patients medication regimens with assistance from a pharmacist.
Prescribing cascades
Patient care can become complex. Multiple chefs in the kitchen, so to speak. Sparse medication reconcilliation. Going from patient to patient. Top it off with a variety of medications on board.
A patient visits reporting swelling in their legs. Patients are unofficially trained to expect a prescription for each concern or at each appointment. They request something to help with the swelling. There’s an easy fix to this – furosemide to the rescue. The swelling subsides, the patient is satisfied.
Eventually the patient returns, this time complaining of frequent urination. They request a prescription to help. Easy enough – one is written for their overactive bladder, oxybutnin. The patient is satisfied. The provider did their job and fixed the problem.
While this scenario is highly simplified, the prescribing cascade continues to expand. Interesting enough, the originating culprit remains in place – the patients current prescription for amlodipine. The swelling was in result to the caclium-channel blocker. The added solution, furosemide, became a culprit as well – frequent urination. The cascade could continue on, unfortunately as urinary incotinence medications have a whirl-wind of possible adverse drug reactions as well.
Pharmacists are trained to watch for this type of scenario. A adequate and fully assessed medication reconcilliation can proactively reduce these cascades. Integrating a pharmacist into the patient-care model can also retroactively assess for appropriateness of therapy of each medication. There continues to be ample opportunity to de-escalate patients medication regimens with assistance from a pharmacist.
Can we put a image with arrows? ????
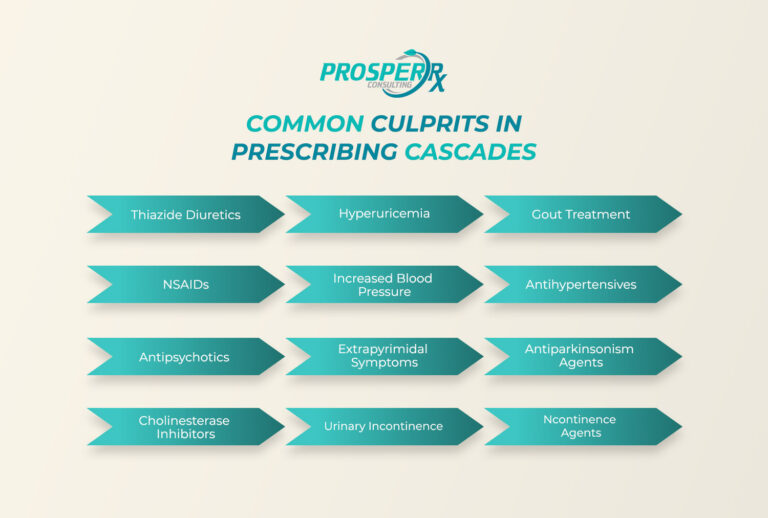
Common culprits in prescribing cascades
Thiazide diuretics –> Hyperuricemia –> Gout treatment
NSAIDs –> Increased blood pressure –> Antihypertensives
Antipsychotics –> Extrapyrimidal Symptoms –> Antiparkinsonism agents
Cholinesterase inhibitors –> Urinary Incontinence –> Incontinence agents